FeatureHospital Airflow Control Technology
In hospital waiting rooms, there is a risk of secondary infection from patients with influenza, COVID-19, and other infections.
Kajima is developing a system—called KIRICA AIR—that uses facial-recognition technology
and thermal cameras to (i) identify people in waiting rooms who are suspected of being infected with a virus that causes infectious diseases
and (ii) control the airflow in the waiting room to minimize the risk of other people inhaling the airborne virus.
KIRICA AIR—a next-generation airflow-control system
that reduces the risk of infection in waiting rooms
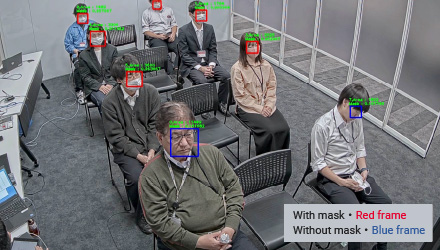
Using facial-recognition technology and thermal cameras
to determine whether someone can be suspected of infection
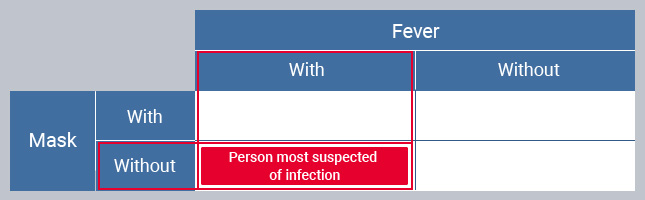
The airflow-control system KIRICA AIR uses (i) facial-recognition technology to determine whether people in the waiting room are wearing masks and (ii) a thermal camera to detect whether they have a fever (high body temperature).
The room occupants who are categorized as “without mask” and “have fever” are judged to be the most likely to be infected, and the other occupants are judged to be the ones who should be protected from infection.
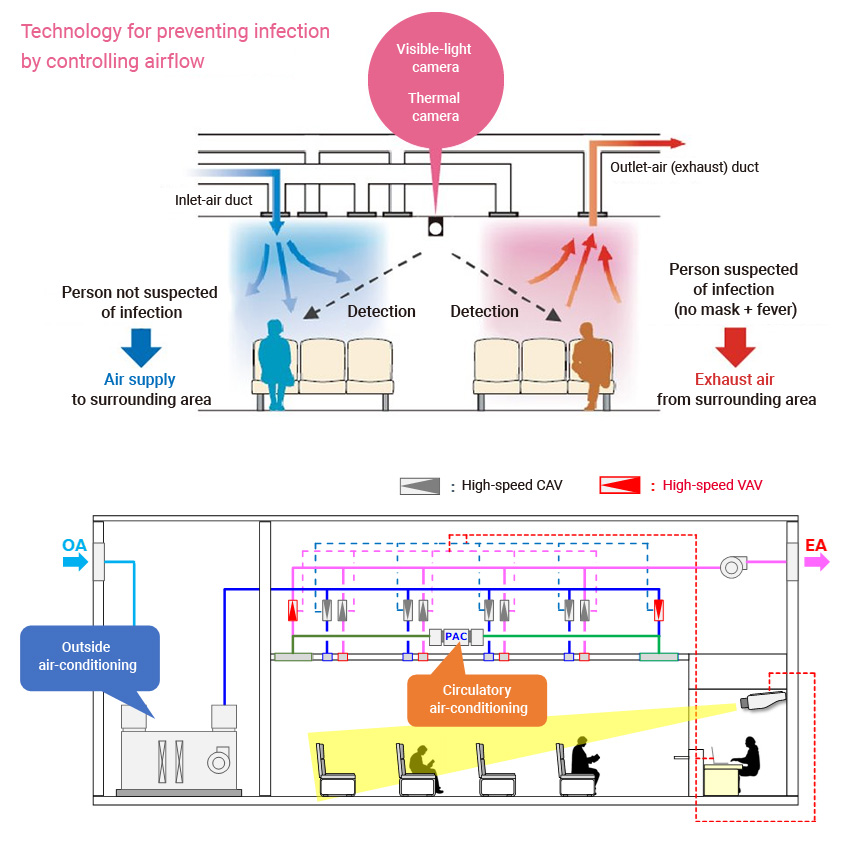
On the basis of these judgements, KIRICA AIR controls the dampers of the variable-air-volume (VAV) system automatically according to the location of people with suspected infection; that is, it adjusts the amount and position of the inflow and outflow air in a way that controls the air flow in the waiting room.
Verifying the effect by air simulation
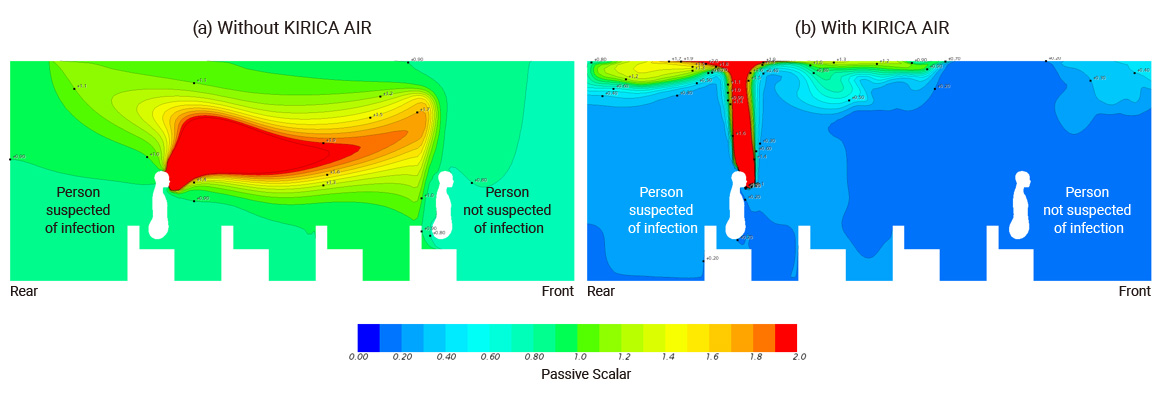
To verify the effectiveness of the KIRICA AIR airflow-control system, a computational fluid dynamics (CFD) analysis model was used to simulate the airflow, and the simulation results were analyzed as described hereafter.
According to the simulation results, as shown in simulation result (a) (below left) when KIRICA AIR was not operating, carbon dioxide (CO2) (assumed to be exhaled breath) exhaled by the infection-suspected person was diffused in the direction of the unsuspected person in the front row of the waiting room. On the contrary, as shown in simulation result (b) (below right), when KIRICA AIR was operating, CO2 emitted by the infection-suspected person diffused mainly upwards, and the CO2 concentration in the front row where the unsuspected person is seated was lower. This result indicates that KIRICA AIR reduces the amount of infected-people-exhaled-virus inhaled by people who are not suspected of infection.
Standardized CO2 concentration simulation
Contributing to countermeasures for
SARS (severe acute respiratory syndrome) and COVID-19
Following the outbreak of SARS (severe acute respiratory syndrome) in 2002, Kajima began research and development focusing on droplets exhaled from infected people. Since then, we have accumulated know-how in evaluating indoor environments, such as recreating hospital rooms in testing facilities and spraying tracer gases such as carbon dioxide (CO2) to measure the efficiency of ventilation and local exhaust ventilation. Furthermore, during the spread of COVID-19, we participated in a “droplet-diffusion project” implemented on supercomputer Fugaku, assisted in simulating droplet diffusion in various architectural spaces, and significantly contributed to COVID-19 countermeasures.
Future developments
From now onwards, countermeasures against new coronaviruses and influenza viruses will continue to be essential, and the emergence of more unknown viruses cannot be ruled out. Kajima will continue its research on building air-conditioning control and contribute to measures against infectious diseases.

